







View this post on Instagram A post shared by Kaiser Raja (@kaiser.raja.md) Autoimmune hepatitis is a rare but serious liver condition where the body’s immune system attacks the liver, causing acute inflammation. ⚠️ Common symptoms:Yellowing of eyes (jaundice), dark urine, itching, fatigue, loss of appetite, and upper abdominal discomfort. It often affects young people, especially […]
Read More
View this post on Instagram A post shared by Kaiser Raja (@kaiser.raja.md)
Read More

3 months post liver transplant and already back on the bike!Philipa’s strength, determination, and spirit are unmatched. Morning rides never looked this powerful. Here’s to health, hope, and unstoppable energy!
Read More
✨ Grateful & Honored ✨ I’m deeply humbled to share that I have been recognized by the Forttuna Global 100 Legacy Makers 2025. What makes this moment even more surreal is seeing my name and photo showcased on a billboard in Times Square, New York. This milestone is not just mine — it reflects the […]
Read More
Kings Liver Support Group Update Today, under the guidance of Dr. Kaiser, we had an insightful one-to-one Q&A session with patients and their families, focusing on life post-transplant and community support. We also had the opportunity to conduct a practical workshop with patients, led by Dr. Kaiser, which added great value to the session. A […]
Read More
Kings Liver Support Group Dubai Dr. Kaiser RajaConsultant in Liver Diseases, Transplant Hepatology, Gastroenterology and Advanced EndoscopyKings College Hospital London Call: +971 4 247 7777 / Whatsapp +971557181328Email: kaiser.raja@kch.aewww.drkaiser.ae
Read More
Celebrating the incredible journey of our post-transplant warrior, Mr. Jasbir Singh, on his special day! 🎉Wishing you endless health, happiness, and success ahead. Here’s to many more milestones and birthdays!Happy Birthday, Jasbir! 🎂✨With Dr. Kaiser & Team*
Read More
In this inspiring journey, Mr. Punjabi a 63-year-old patient underwent a life-saving liver transplant at King’s College Hospital Dubai. From the initial diagnosis of liver cirrhosis, early-stage cancer, and additional health challenges like advanced heart disease, Mr. Punjabi’s story is a testament to the expert medical care at King’s Liver Transplant Centre of Excellence, and […]
Read More
Certificate of Appreciation: Health Screening and Awareness Camp held on 26th July 2025 at AG Marbles, Al Quoz. Dr. Kaiser RajaConsultant in Liver Diseases, Transplant Hepatology, Gastroenterology and Advanced EndoscopyKings College Hospital Dubai Call: +971 4 247 7777Whatsapp +971557181328Email: kaiser.raja@kch.aewww.drkaiser.ae
Read More
King’s College Hospital London in Dubai has successfully completed 14 liver transplants within the first year of launching Dubai’s first adult liver transplant centre. This milestone was recently celebrated during an event at the hospital, attended by senior hospital officials, as well as medical and nursing staff.
Read More
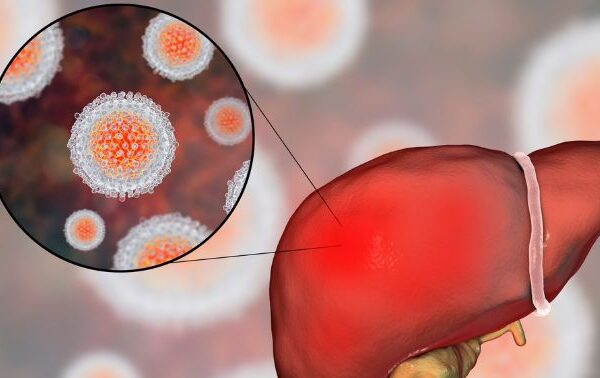
The Silent Epidemic: What You Don’t Know Can Hurt You Millions of people around the world are living with hepatitis and don’t even know it. Hepatitis B and C — two of the most common forms — often show no symptoms until the disease is advanced. Every year, over 3 million new cases are reported, […]
Read More
We are proud to introduce Dubai’s first dedicated Paediatric and Adult Liver Transplant Centre, marking a pivotal chapter in a legacy of over 40 years of pioneering liver care!
Read More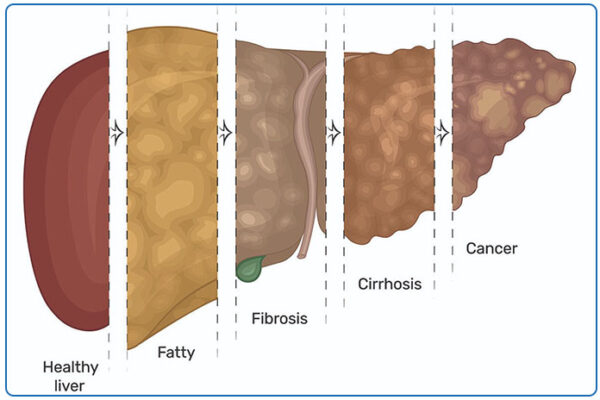
The most common cause of chronic liver disease. Usually causes no symptoms. Can progress to liver cirrhosis. Fatty liver is an extremely common condition usually detected incidentally on an ultrasound scan. It develops in individuals who are overweight, and in those with diabetics. Even people with mild obesity and especially abdominal obesity are prone to […]
Read More
🩺✨ Join Us at the 5th Annual Dubai International Gastroenterology Congress!📅 Date: 24–25 May 2025📍 Location: Dubai, UAE 🎙️ Featured Speaker:Dr. Kaiser RajaConsultant in Gastroenterology & Liver DiseaseKing’s College Hospital, UAE 🧠 Topic: Management of Decompensated Cirrhosis: What’s New
Read More
Alcoholic liver disease is a result of overconsuming alcohol that damages the liver, leading to accumulation of fat in the liver, inflammation, and scarring. It can lead to cirrhosis and can be fatal. Most individuals who consume excessive alcohol may not be aware of ongoing liver damage. We recommend a comprehensive evaluation of liver disease, including […]
Read More
A Morning of Strength, Support and Steps! 🚶🚶♀️🚶♂️ What a fantastic start to the day for our Liver Transplant Support Group! Together, they walked 4 km and took 6,750 steps filled with positivity and resilience along Dubai Marina. We look forward to this becoming a weekly tradition for health, connection, and encouragement! Dr. Kaiser RajaConsultant […]
Read More
[vc_row css=”.vc_custom_1703148958767{padding-right: 0px !important;padding-left: 0px !important;background-color: #edf2fb !important;}”][vc_column][vc_empty_space height=”22px”][/vc_column][/vc_row][vc_row css=”.vc_custom_1703148966780{padding-right: 0px !important;padding-left: 0px !important;background-color: #edf2fb !important;}”][vc_column][vc_single_image image=”7455″ img_size=”full” alignment=”center”][vc_empty_space height=”22px”][vc_custom_heading text=”Our First Liver Transplant at King’s College Hospital London in Dubai, United Arab Emirates” font_container=”tag:h5|text_align:left|color:%230a2544″ use_theme_fonts=”yes”][vc_empty_space height=”10px”][vc_column_text]Our Liver Team at King’s College Hospital performed the first liver transplantation in the Emirate of Dubai. The fortunate […]
Read More
Guests of Honour for the Forttuna Global Excellence Awards 2024! Dr. Kaiser Raja – Director of the Hepatology And Liver Transplantation Program at King’s College Hospital London, UAE
Read More
Join us as we delve into the revolutionary Role of Endoscopic Ultrasound in Hepatology and Liver Diseases with the distinguished Dr. Kaiser Raja from King’s College Hospital London, UAE! 🏥✨ 🔍 Discover how cutting-edge endoscopic ultrasound is transforming the diagnosis and management of complex liver conditions.💡 Gain insights into the latest advancements in liver disease […]
Read More
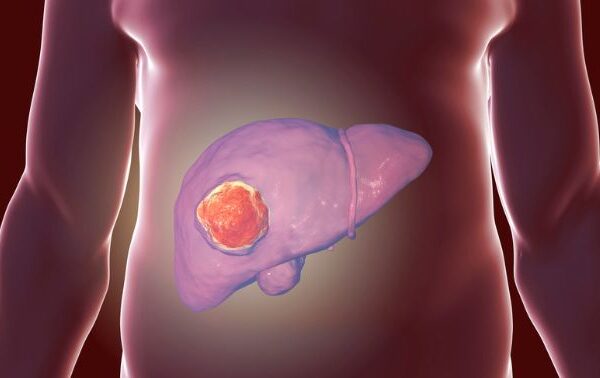
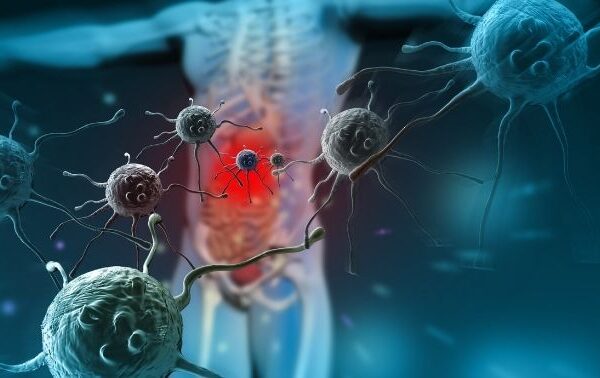
October is Liver Cancer Awareness Month, which is a chance to raise vital awareness to improve early detection of the disease as well as showing support for people affected by liver cancer and remember loved ones.
Read More
Dr. Kaiser Raja, Consultant in Liver Diseases, Transplant Hepatology, Gastroenterology and Advanced EndoscopyKings College Hospital London
Read More
This is a form of inflammatory disease affecting the colon. It leads to loose stools often mixed with blood. A colonoscopy is needed for diagnosis. There are good long term treatment options and the disease can be controlled very well. Newer biological drugs have completely changed the treatment landscape. You can contact us in case […]
Read MoreMr.Tahir suffered from a severe liver problem called liver cirrhosis for over four years. Unfortunately, a liver transplant was not something that was accessible to him. Mr Tahir and his family sought out help from many hospitals and foundations without any luck. Thankfully, he came to King’s where we were able to assess him and […]
Read More
Watch as Dr Kaiser Raja, talks about all things Liver and the first successful Liver Transplant in Dubai right here at King’s College Hospital Dubai. If you have any questions please fell free to contact with us.
Read More
View this post on Instagram A post shared by Kaiser Raja (@kaiser.raja.md) We are proud to announce that we have completed 6 successful liver transplantations. A huge thank you to our excellent liver transplant centre team and to the donors and their families who’s selfless decisions have changed lives!
Read More
Liver Transplant Support Group Join our upcoming Liver Transplant Support Group meeting a supportive space for recipients, caregivers, and family to connect and share experiences. Let’s Join UsJuly 25th, 2024 05.00 PM – 07.00 PMKings College Hospital LondonDubai, Dubai Hills. Location:https://maps.app.goo.gl/cB44iA8ns4J1oroe6
Read More
The Bravery Blueprint: Dr. Kaiser Raja | FFTB 02 – Dr. Kaiser Raja x Raul Handa | The FFTB Show Dr. Kaiser RajaConsultant in Liver Diseases, Transplant Hepatology, Gastroenterology and Advanced EndoscopyKings College Hospital London Call: +971 4 247 7777 / Whatsapp +971557181328 Email: kaiser.raja@kch.ae www.drkaiser.ae Location:https://maps.app.goo.gl/cB44iA8ns4J1oroe6
Read More
May is Hepatitis Awareness Month in the U.S. Globally, 354 million people live with viral hepatitis in the world today Every year, more than a million lives are lost to hepatitis. We’re not waiting for change – we’re fighting to make it happen. more than 1.2 Million lives are lost each year to hepatitis B and […]
Read More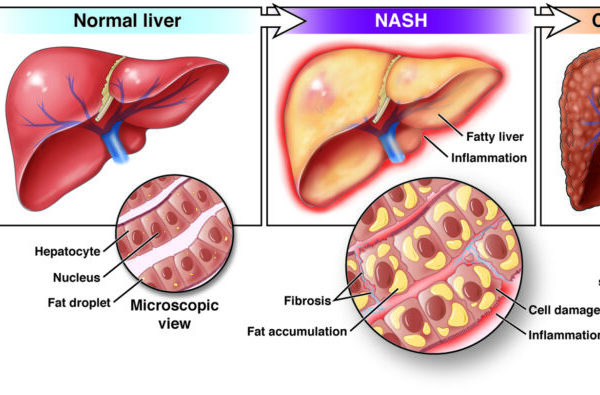
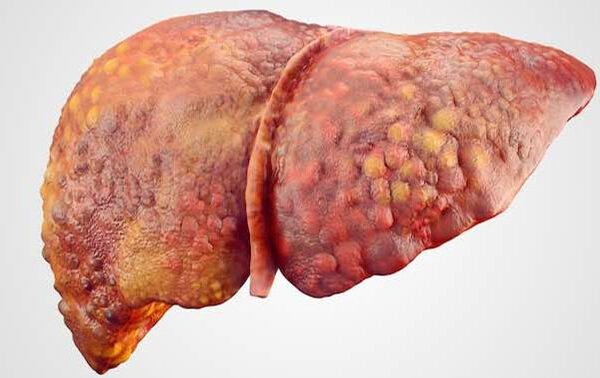
Extreme liver fibrosis is known as liver cirrhosis. In this condition, the liver which is otherwise a soft organ becomes quite hard and starts functioning poorly. Patients can go on to develop liver failure in which there is development of jaundice (yellow eyes), generalized weakness, loss of muscle mass, accumulation of fluid in the belly […]
Read More
This is the most important differentiation to be made when a patient seeks medical consultation for fatty liver. Simple fatty liver usually does not progress to advanced liver disease while NASH may progress over several years to more advanced forms of liver disease such as liver fibrosis and cirrhosis. Advanced NASH is also a risk […]
Read More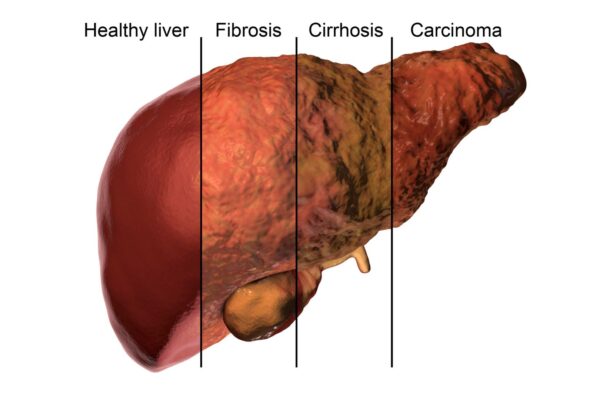
Fatty liver usually develops in individuals who are overweight, and in those with diabetics. Even people with mild obesity and especially abdominal obesity are prone to develop fatty liver. Fatty liver is especially common in those with a condition called metabolic syndrome. Patient with metabolic syndrome usually have a combination of one of more of […]
Read More
Simple fatty liver without liver inflammation (also known as nonalcoholic fatty liver or NAFL). This is generally a benign condition that usually does not progress to advanced forms of liver disease. Fatty liver with liver inflammation (also known as non-alcoholic steato-hepatitis or NASH). In this condition, the excess fat in the liver causes inflammation of […]
Read More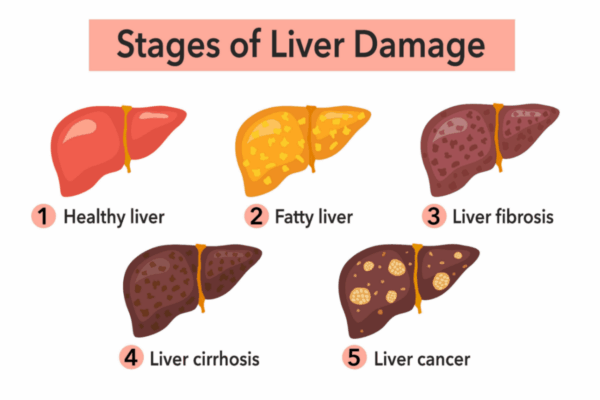
Fatty liver disease is a medical condition in which there is accumulation of excess fat in the liver. Fatty liver has been well known to be associated with excess alcohol consumption. But Fatty Liver is also extremely common in individuals who do not drink alcohol or drink little alcohol. This form of fatty liver is […]
Read More
World Liver Day is celebrated globally on April 19. The day focuses on increasing awareness of liver-related problems and diseases. The liver is one of the vital organs, responsible for immunity, digestion, and metabolism. Any liver disease or sickness affects not only the digestive system, but also the kidneys, lungs, heart, and brain. Excess fat […]
Read More
A colonoscopy is an examination of the inside of the large intestine, which includes the entire colon, rectum and anus. It is a type of endoscopy, in which a flexible tube with a camera at one end (colonoscope) is inserted into your body. The colonoscope passes through your anus and rectum into your colon. This is […]
Read More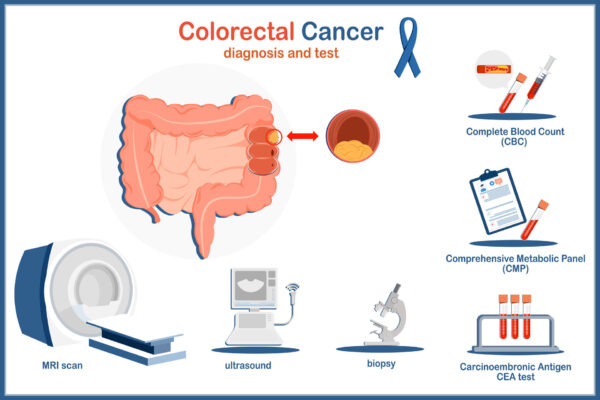
Screening involves direct visualization of the inner lining of the colon to detect polyps. This can be done either by colonoscopy or sigmoidoscopy. Non-invasive techniques such as virtual colonoscopy using a CT scan can also visualize the colon lining. Other colon cancer screening tests involve stool analysis for presence of occult blood which may indirectly […]
Read More
Role of Endoscopic Ultrasound in Hepatology/Liver Diseases International Conference on Advances in Gastroenterology and HepatologyGastroenterology 2024 Multidisciplinary Approaches to Digestive Health: Collaborating for Better Outcomes April 19-20, 2024, Dubai, UAE
Read More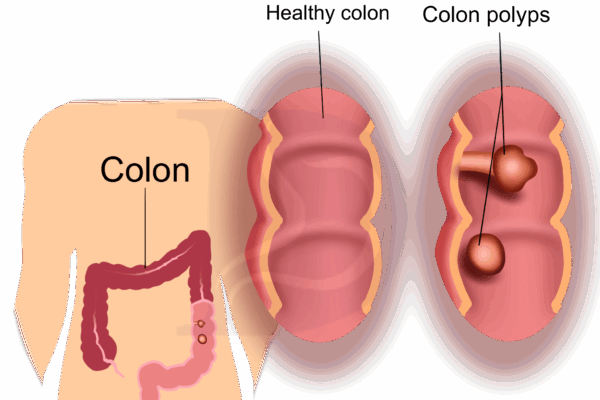
[vc_row][vc_column][vc_custom_heading text=”What are colon polyps and why should you look for them?” font_container=”tag:h5|text_align:left|color:%231e73be” google_fonts=”font_family:Prata%3Aregular|font_style:400%20regular%3A400%3Anormal”][vc_empty_space][vc_empty_space height=”10px”][/vc_column][/vc_row][vc_row][vc_column width=”1/2″][vc_custom_heading text=”What are colon polyps?” font_container=”tag:h5|text_align:left” use_theme_fonts=”yes”][vc_column_text]A colon polyp is a growth on the inner lining of the colon (large intestine) or rectum. Polyps in the colon arise from uncontrolled multiplication of cells leading to growth of tissue. This can […]
Read More
Most colon polyps and early colorectal cancer do not have any symptoms, which is why screening is recommended. However, when symptoms do occur, they may include:
Read More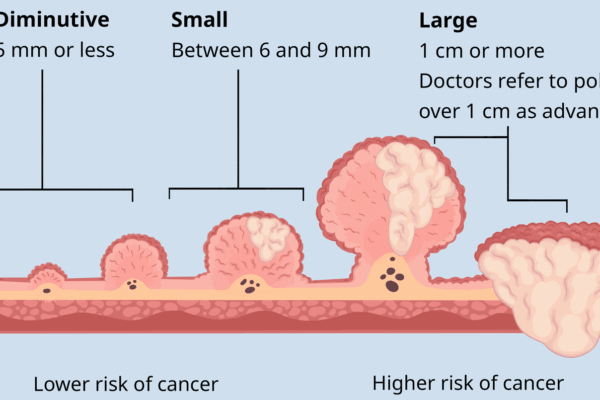
Essentially there are two types of polyps. Hyperplastic polyps which are not pre-cancerous and adenoma type of polyps which are pre-cancerous. The type of the polyp can be determined only after its removal.
Read More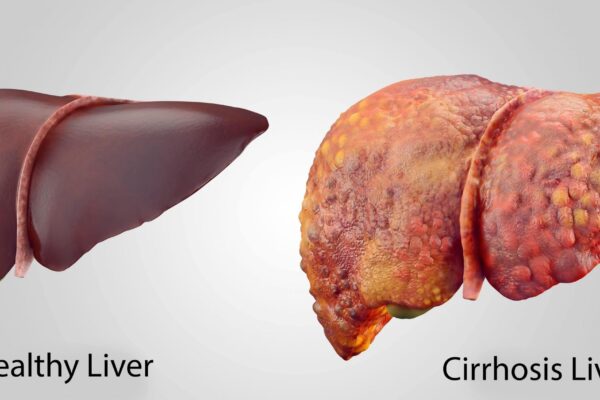
The three most common diseases that cause chronic liver disease, liver fibrosis and cirrhosis are alcoholic liver disease, chronic viral hepatitis (hepatitis B and C), and non-alcoholic fatty liver disease that is usually associated with diabetes and obesity. Other diseases such as autoimmune hepatitis, and excess of iron in the body known as hemochromatosis can […]
Read More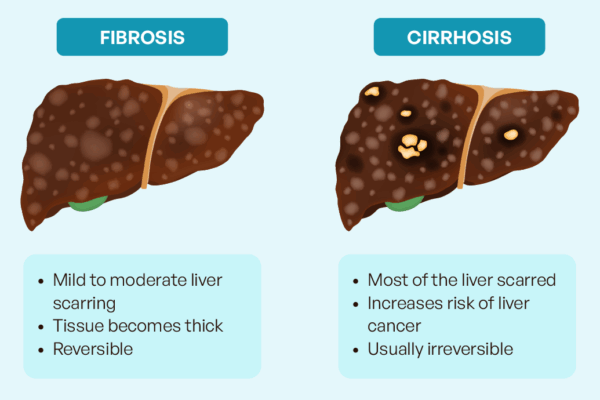
Liver fibrosis does not cause any symptoms and routine blood tests and ultrasound scan cannot detect liver fibrosis. It is important to detect liver fibrosis at an early stage so that its progression can be prevented. If untreated, liver fibrosis may progress to cirrhosis of the liver, liver failure, and liver cancer. If you have […]
Read More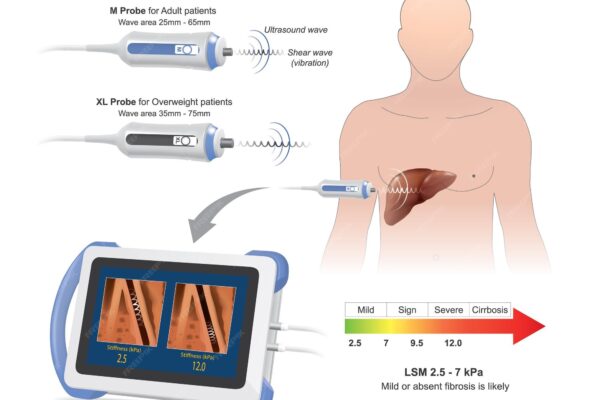
Fibroscan uses ultrasound waves using a technique called transient elastography. Liver stiffness is evaluated by measuring the speed of a vibration wave as it travels through the liver. The speed of the vibration wave is slower in a soft (normal) liver and faster in a firm or hard (fibrotic) liver. Liver stiffness is eventually expressed […]
Read More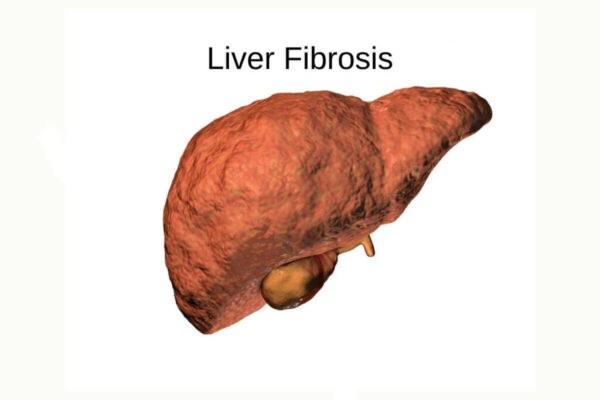
Many chronic liver diseases such as fatty liver, hepatitis B, hepatitis C, or excessive alcohol use can cause persistent inflammation of the liver and lead to progressive liver damage. Over a period or time, healthy liver tissue is replaced by scars. Scarring of the liver is known as liver fibrosis. Liver fibrosis results in diminished […]
Read More
It is recommended not to eat or drink anything for three hours before the Fibroscan. If needed, you can have small sips of water or clear fluid. You will be asked to lie flat on your back on an examination couch and to place your right arm behind your head. The examiner will feel the […]
Read More
The complex, four-hour-long surgery involved the complete removal of the diseased liver and the implantation of a healthy one The first liver transplant in Dubai recently took place at Kings College Hospital London- Dubai. The patient, a 38-year-old woman, suffered from a rare condition known as autoimmune hepatitis, which causes the body’s immune system to […]
Read More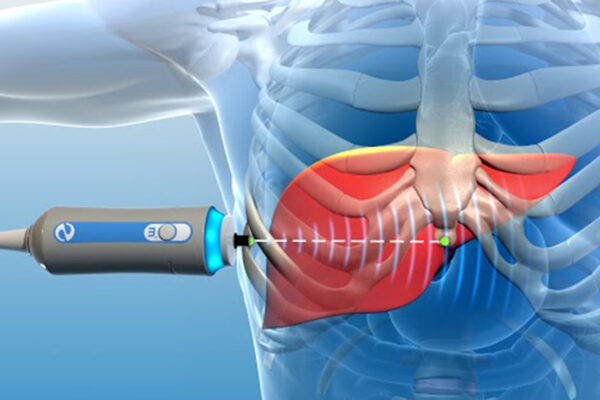
A Fibroscan is a type of scan that measures the ‘stiffness’ of your liver, which in turn reflects the degree of scarring (fibrosis) in your liver. It is a simple, painless test which gives immediate results. It does not have any potential complications or risks and is non-invasive, which means that it does not break […]
Read More
Wishing you and your family A Happy New Year filled with hope, health, and happiness.
Read More

The UAE National Day is celebrated yearly on 2 December to commemorate the formation of the United Arab Emirates.
Read More
Clinics in Liver DiseasesAutoimmune Hepatitis and Cholestasis: Current Knowledge and Clinical PracticeCase Presentations and Discussion Speaker Dr. Kaiser RajaConsultant in Gastroenterology and HepatologyKCH Liver Care and Transplant ProgramKing’s College Hospital London, Dubai Date: THURSDAY 30th November 2023Time: 08:30 PM – 10:00 PM (Dubai Time)Venue: JW Marriott Marquis Hotel Dubai 04 519 9999 / 971557181328Email: kaiser.raja@kch.ae
Read More
Did you know that Diabetes is one of the major risk factor fatty liver and liver fibrosis. If you are a diabetic, make sure you have checked for liver disease. A simple FIB-4 test and Fibroscan are easy ways to check for liver disease. If you have any questions please fell free to contact with […]
Read More
May millions of lamps illuminate your life with endless prosperity, health, and wealth forever. Wishes you and your family a Very Happy Diwali
Read More